

Abstract
Objective. The probability of achieving Clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) treatment targets (remission [REM], low disease activity [LDA]) was evaluated following apremilast monotherapy in disease-modifying antirheumatic drug (DMARD)-naïve patients with psoriatic arthritis (PsA) based on baseline disease activity.
Methods. This post hoc probability analysis of PALACE 4, a phase III, multicenter, randomized, placebo-controlled study, evaluated shifting across cDAPSA categories from baseline to week 52 and included DMARD-naïve patients receiving apremilast 30 mg BID with available baseline cDAPSA data. Changes in articular/extraarticular manifestations were evaluated in patients with week 52 cDAPSA components. cDAPSA treatment target achievement was assessed in a subgroup with baseline extraarticular PsA manifestations (skin involvement, enthesitis, dactylitis).
Results. Of 175 apremilast-treated patients in the probability analysis, 66.3% were in high disease activity (HDA) and 31.4% in moderate disease activity (ModDA) at baseline. Approximately twice as many patients in ModDA at baseline reached REM/LDA at week 52 vs those in HDA (61.7% vs 28.2%). Achieving cDAPSA treatment targets was associated with reductions in articular (swollen/tender joints) and extraarticular (skin involvement, enthesitis, dactylitis, functional disability) disease activity. Similar treatment target achievement rates were observed in the subgroup with ≥ 1 extraarticular PsA manifestation (n = 126; ModDA: 66.7%, HDA: 32.2%).
Conclusion. Apremilast-treated patients with baseline ModDA had higher probability of achieving cDAPSA treatment targets than patients with HDA. Resolution and/or near resolution of articular and/or extraarticular PsA manifestations was achieved by patients in REM/LDA at week 52. Consistent treatment target achievement was observed in patients with 1 or multiple extraarticular manifestations of active PsA.
Psoriatic arthritis (PsA) is a chronic inflammatory disease associated with manifestations and comorbidities that can significantly impair quality of life.1 The oral phosphodiesterase 4 inhibitor apremilast modulates inflammatory mediators and is approved for the treatment of patients with PsA.2,3 In the phase III PALACE 1–4 studies, apremilast was associated with significant American College of Rheumatology response rates in patients with PsA who were naïve to or had experience with disease-modifying antirheumatic drugs (DMARDs).2,4,5,6,7 The benefits of earlier treatment for PsA are known,8,9,10 and recent guidelines promote a treat-to-target approach for PsA with a goal of remission (REM) or low disease activity (LDA).11 Apremilast was associated with achievement and maintenance of the commonly used Clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) treatment targets in DMARD-experienced patients with moderate disease activity (ModDA) in the PALACE 1–3 studies.12 Whether DMARD-naïve patients treated with apremilast have greater chances of achieving cDAPSA treatment targets than DMARD-experienced patients is unknown. It is often assumed that patients with less treatment experience tend to have less disease burden, but the DMARD-naïve patients in PALACE 4 had substantial active disease and burden.7 In addition, whether specific manifestations other than arthritis (skin involvement, enthesitis, and dactylitis) have an effect on the achievement of cDAPSA treatment targets in this patient population is unknown.
We assessed the predictive value of baseline clinical disease status for achievement of long-term cDAPSA treatment targets at week 52 among DMARD-naïve patients, both overall and within a subgroup, who also had extraarticular manifestations of PsA in addition to peripheral joint involvement in PALACE 4. The cDAPSA tool indirectly captures severity assessments of PsA manifestations such as enthesitis, dactylitis, functional status, and skin involvement. Therefore, to complement the predictive analyses, we also assessed whether achievement of cDAPSA disease targets with apremilast in DMARD-naïve patients in the overall PALACE 4 population was associated with no or mild disease activity in these domains by week 52 in the subset of patients who had these manifestations.
METHODS
Study population. Detailed inclusion and exclusion criteria for the PALACE 4 study have been previously published.7 Briefly, eligible adults with active PsA for ≥ 3 months who met the Classification Criteria for Psoriatic Arthritis (CASPAR) and had ≥ 3 swollen and ≥ 3 tender joints13 with no prior treatment with conventional synthetic DMARDs or biologics were enrolled in PALACE 4. Stable doses of oral glucocorticoids and nonsteroidal antiinflammatory drugs (NSAIDs) were permitted before study entry. PALACE 4 was conducted in accordance with the general ethical principles of the Declaration of Helsinki and the study protocol was approved by the Schulman Associates Institutional Review Board (OMB No. 0910-0014). Informed written consent was obtained from each patient prior to any study-related procedure.
Study design. The study design for PALACE 4 (ClinicalTrials.gov: NCT01307423) has been previously described.7 Briefly, this phase III, multicenter, randomized, double-blind, placebo-controlled trial randomized 527 patients (1:1:1) to receive apremilast 30 mg BID, apremilast 20 mg BID, or placebo BID. Patients whose swollen and tender joints did not improve by at least 20% by week 16 (early escape) were rerandomized to apremilast 30 mg BID or 20 mg BID if they were initially randomized to placebo or remained on their initial apremilast dose if they were initially randomized to apremilast. At week 24, all patients remaining on placebo were rerandomized to receive apremilast 30 mg BID or 20 mg BID.
The current post hoc analysis includes 175 patients who were randomized to receive apremilast 30 mg BID (regulatory approved dose) at baseline and had cDAPSA data available. One patient was missing cDAPSA component data at baseline and was excluded from the probability analysis. A subgroup analysis among patients who also exhibited any of the extraarticular manifestations, including psoriasis-involved body surface area ≥ 3%, Maastricht Ankylosing Spondylitis Enthesitis Score (MASES) > 0, and/or dactylitis count > 0 at baseline, was also conducted. Patients were divided into 4 subgroups based on the number of manifestations exhibited: ≥ 1, only 1, any 2, or all 3.
Endpoints. The cDAPSA is a composite of the swollen joint count (SJC) and tender joint count (TJC), patient assessment of pain (PAP), and patient global assessment of disease activity (PtGA).14 Probabilities of shifting across different cDAPSA categories (REM: ≤ 4; LDA: > 4 to ≤ 13; ModDA: > 13 to ≤ 27; high disease activity [HDA]: > 27) from baseline to week 52 were calculated in the overall population, and disease activity at baseline and weeks 16, 24, 40, and 52 was assessed according to cDAPSA category at week 52. Treatment goals were achievement of cDAPSA REM or LDA. In the subgroup of patients stratified by extraarticular PsA manifestations at baseline, the proportions of patients who shifted from ModDA or HDA at baseline to treatment targets of REM or LDA at week 52 were calculated.
Mean values of articular and extraarticular variables from baseline to week 52 were assessed by cDAPSA category state at week 52 in the overall population to determine the association between achievement of treatment targets and control of articular and extraarticular manifestations. Articular variables included SJC and TJC; extraarticular variables included enthesitis, dactylitis, Health Assessment Questionnaire–Disability Index (HAQ-DI), and skin involvement.
Statistical analysis. The probability of achieving treatment targets for different baseline clinical disease categories was assessed through the shifting of cDAPSA categories from baseline to week 52 using the longitudinal data of the overall population. Missing data, including discontinuations, were imputed using multiple imputation (repeated 30 times) based on continuous cDAPSA data. Categorization of cDAPSA was implemented according to the categories defined above. Similar assessments using data as observed were performed for the subgroup with extraarticular PsA manifestations.
Using data as observed over time, longitudinal analyses assessing the control of articular and extraarticular domains associated with the achievement of cDAPSA response categories were performed for patients who had cDAPSA components available at week 52 to complement the predictive value analyses. Results are presented according to cDAPSA categorical responses (REM, LDA, ModDA, and HDA) at week 52. The goodness of fit was examined, and the data were, in general, normally distributed except in cases where the sample size was small.
RESULTS
Baseline demographics and characteristics. A total of 175 DMARD-naïve patients in the PALACE 4 study who were randomized to apremilast 30 mg BID at baseline and had baseline cDAPSA component data were included in the probability analysis. At baseline, 66.3% (116/175) of patients were in HDA, 31.4% (55/175) were in ModDA, and 2.3% (4/175) were in LDA.
Of this population, 138 patients had all 4 cDAPSA components available at week 52 and were included in the longitudinal analyses. Baseline demographics and clinical characteristics for these patients categorized by week 52 cDAPSA categories are presented in Supplementary Table 1 (available with the online version of this article). Mean duration of PsA was 1.5 to 4.6 years across groups; patients had active disease, as shown by cDAPSA, SJC, TJC, MASES, and dactylitis count. Baseline study population characteristics such as mean age, BMI, and baseline NSAID use were generally similar across week 52 cDAPSA categories, although patients in HDA at week 52 had a higher mean BMI at baseline. Despite higher baseline disease activity in the ModDA and HDA groups at week 52, baseline HAQ-DI scores were similar across week 52 cDAPSA categories.
Of the 175 patients with baseline cDAPSA component data, 10 did not have any extraarticular PsA manifestations, resulting in 165 patients with ≥ 1 extraarticular PsA manifestation (ie, skin involvement/enthesitis/dactylitis) at baseline. Of these, 54 patients had only 1 extraarticular PsA manifestation, 84 had 2, and 27 had all 3. The study population with at least 1 manifestation had a mean age of 48.8 years, PsA duration of 3.6 years, Psoriasis Area and Severity Index (PASI) score of 6.6, MASES of 3.8, and dactylitis count of 3.5 (Supplementary Table 2, available with the online version of this article). Mean cDAPSA at baseline was 39.4 (corresponding to HDA on the group level), and baseline mean values for cDAPSA components were 10.3 (SJC), 18.5 (TJC), 52.8 (PAP), and 53.8 (PtGA). The subgroup analysis included 130 patients with ≥ 1 extraarticular PsA manifestation at baseline and cDAPSA data available at week 52. Within this subgroup, 31.5% (41/130) of patients had 1 of the 3 extraarticular PsA manifestations, including 17 with skin involvement only, 7 with dactylitis only, and 17 with enthesitis only. Among those with ≥ 2 extraarticular manifestations, 51.5% (67/130) had any 2 of the 3, and 16.9% (22/130) had all 3. At baseline, 69.2% of patients in the subgroup with ≥ 1 extraarticular PsA manifestation were in HDA, 27.7% were in ModDA, and 3.1% were in LDA, similar to the overall population. The proportion of patients in HDA at baseline was numerically higher among those with 2 (73.1% [49/67]) or 3 (81.8% [18/22]) manifestations than among those with only 1 (56.1% [23/41]).
Achievement of treatment goals. In the overall PALACE 4 population, the baseline cDAPSA category was found to predict treatment outcomes at week 52 in the PALACE 4 study population, with patients in ModDA at baseline twice as likely to achieve treatment goals (REM/LDA) vs patients in HDA at baseline (61.7% vs 28.2%, respectively; Figure 1). In patients in ModDA at baseline who achieved REM at week 52, mean cDAPSA was 11.9 at week 16, signaling early LDA response in these patients.

Probability of achieving Clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) targets at week 52 by baseline cDAPSA category (n = 175). Multiple imputation used for missing data. HDA: high disease activity; LDA: low disease activity; ModDA: moderate disease activity; REM: remission.
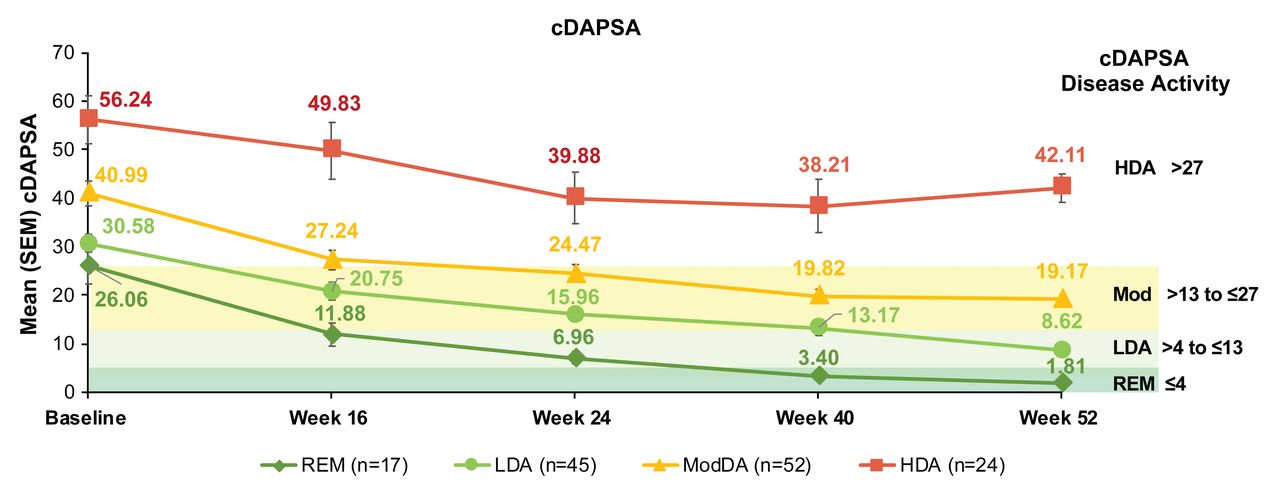
Figure 2 presents the longitudinal assessment of disease activity (mean cDAPSA) over 52 weeks according to cDAPSA categories at week 52. PALACE 4 DMARD-naïve patients who achieved treatment targets at week 52 had lower mean cDAPSA values at baseline and continuous improvements in disease activity.
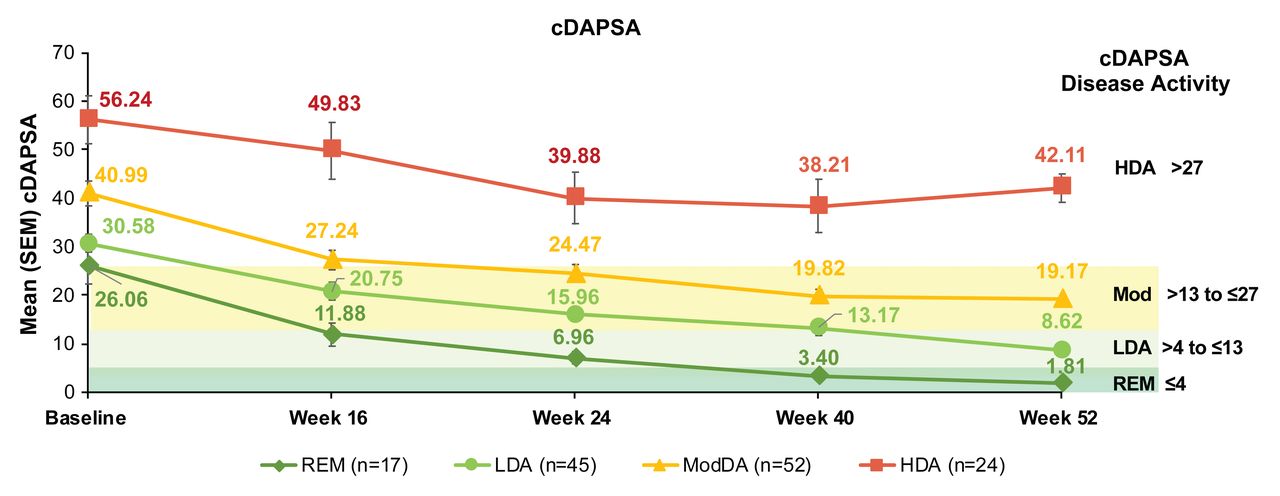
Overall disease activity by Clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) category at week 52. Data as observed. HDA: high disease activity; LDA: low disease activity; ModDA: moderate disease activity; REM: remission; SEM: standard error of the mean.
Changes in articular and extraarticular disease manifestations in the overall PALACE 4 population. Patients in PALACE 4 who achieved cDAPSA treatment targets of REM or LDA at week 52 showed no or mild arthritic disease activity by week 52, as measured by SJC and TJC (Supplementary Figure 1, available with the online version of this article). Similarly, a greater decrease in measures of extraarticular disease activity, including MASES, dactylitis count, HAQ-DI, and PASI scores, was observed in patients achieving cDAPSA treatment targets at week 52 (Supplementary Figure 2).
Achievement of treatment goals. Within the subgroup of 130 patients with ≥ 1 extraarticular manifestation at baseline, 4 were in LDA at baseline and were not included in the subgroup analysis. Among the remaining 126 patients, a greater proportion of those with ModDA achieved REM/LDA at week 52 than patients with HDA (66.7% vs 32.2%; risk difference: 0.34; Figure 3), similar to results from the overall population (Figure 1). This pattern was consistent regardless of how many extraarticular manifestations were present (Figure 3). Among patients with only 1 extraarticular manifestation, 72.2% of those in ModDA at baseline achieved REM/LDA at week 52 vs 39.1% of those in HDA (risk difference: 0.33). In patients with any 2 manifestations, 57.1% of those in ModDA at baseline achieved treatment targets vs 28.6% of those in HDA (risk difference: 0.29). Similarly, in patients with all 3 extraarticular manifestations, a greater proportion of patients with ModDA achieved treatment targets at week 52 than those with HDA (75.0% vs 33.3%; risk difference: 0.42).
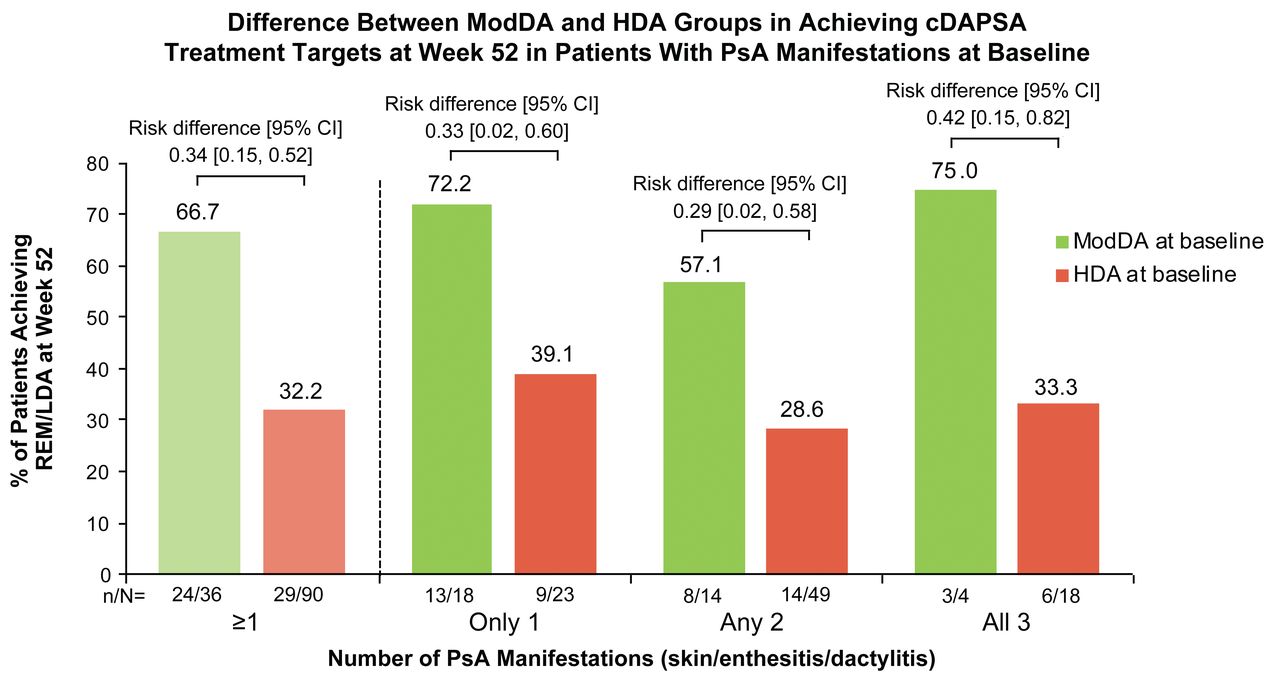
Proportions of patients achieving Clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) treatment targets in patients with ≥ 1 PsA manifestation at baseline. Data presented are observed cases. Category of “≥ 1” contains all patients in categories of “only 1,” “any 2,” or “all 3, which are mutually exclusive.” HDA: high disease activity; LDA: low disease activity; ModDA: moderate disease activity; PsA: psoriatic arthritis; REM: remission.
DISCUSSION
Apremilast-treated, DMARD-naïve patients with PsA in PALACE 4 had substantial baseline disease activity, particularly for disease activity domains such as SJC, TJC, enthesitis, and dactylitis.7 The disease activity reported here (ModDA: 31.4%; HDA: 66.3%) was similar to that observed in DMARD-experienced patients in the PALACE 1–3 studies (ModDA: 24.5%; HDA: 74.3%),12 suggesting disease burden that is potentially higher than expected in this DMARD-naïve population.
A total of 97.7% of the PALACE 4 DMARD-naïve patients had ModDA or HDA at baseline. Although a portion of patients with HDA at baseline achieved treatment targets of cDAPSA REM or LDA by week 52 with continued apremilast treatment (28.2%), patients in ModDA at baseline had a greater likelihood of achieving treatment targets (61.7%). These findings were similar to those observed in the PALACE 1–3 DMARD-experienced patient population, in which achievement of treatment targets was twice as likely in the group with ModDA vs HDA at baseline (46.9% vs 24.9%).12 This pattern also held true for patients in the subgroup with skin involvement, enthesitis, and/or dactylitis at baseline, with greater proportions of those in ModDA at baseline attaining cDAPSA REM or LDA at week 52 of apremilast treatment than patients in HDA. This observation was consistent regardless of whether patients had only 1 PsA manifestation or multiple PsA manifestations. Patients receiving apremilast who achieved cDAPSA treatment targets also experienced improvements in extraarticular manifestations of PsA, such as skin involvement, enthesitis, dactylitis, and functional disability by week 52, further supporting previous findings on the validity of using cDAPSA as a simple tool for following disease activity in patients with PsA. Moreover, these manifestations did not prevent or reduce the possibility of achieving the treatment targets of REM or LDA.
Treatment guidelines emphasize the importance of REM or LDA as a treatment target.11 Results from the current analyses provide valuable insights regarding attainment of treatment targets in DMARD-naïve patients with PsA in ModDA receiving apremilast, particularly when considered in the context of an equivalent analysis in the PALACE 1–3 DMARD-experienced patient population. Additionally, these results provide insight into achievement of treatment targets in patients with extraarticular manifestations of PsA. While traditional assessments use baseline data to predict outcomes, a modern approach using endpoint data has been successfully utilized for various treatment strategies over the past decade.15,16 Using longitudinal disease activity data (mean cDAPSA) according to cDAPSA categories at week 52 provides population-level data that complements the individual patient analysis by baseline disease activity group. The baseline values of patients achieving week 52 treatment targets may help to identify patient characteristics indicative of treatment response and thereby help to inform treatment decisions.
A limitation of controlled clinical studies is the enrollment of highly selected patients with restricted eligibility criteria, which may not be representative of patients with PsA treated in real-world clinical settings. The PALACE 4 population may not be reflective of the early, treatment-inexperienced PsA population; although patients in PALACE 4 were DMARD-naïve, many had longstanding disease. A further limitation of the study is the use of MASES for the assessment of enthesitis. Enthesitis assessments such as the Spondylarthritis Research Consortium of Canada and Leeds Enthesitis Index measure multiple peripheral enthesitis sites. MASES measures peripheral enthesitis only in the Achilles tendon.17 However, peripheral enthesitis occurring in other sites may have been indirectly captured through the cDAPSA, which provides an assessment of overall disease activity.
Our findings demonstrate that baseline disease activity, as measured by the cDAPSA, is a predictor of achievement of treatment targets in DMARD-naïve patients following apremilast treatment. Further, patients achieving treatment targets at week 52 had lower mean cDAPSA values at baseline and continuous improvements in disease activity. Importantly, greater proportions of patients in ModDA at baseline who exhibited extraarticular manifestations of PsA achieved REM/LDA at week 52 than patients in HDA, suggesting these manifestations do not prevent achievement of cDAPSA REM/LDA. Achievement of cDAPSA treatment targets was also associated with greater improvements in extraarticular disease aspects not captured in the cDAPSA by week 52. Overall, this study supports apremilast as an effective treatment for DMARD-naïve patients with PsA regardless of the presence of extraarticular manifestations of the disease.
ACKNOWLEDGMENT
The authors thank Michele Brunori, formerly of Amgen Europe GmbH, for his contributions to the study. Writing support was funded by Amgen Inc. and provided by Kristin Carlin, BSPharm, MBA, of Peloton Advantage, LLC, an OPEN Health company, and Cathryn M. Carter, MS, employee of and stockholder in Amgen Inc.
Footnotes
This study was sponsored by Amgen Inc.
PJM has received grant/research support from and served as a consultant for AbbVie, Amgen, Boehringer Ingelheim, BMS, Celgene, Eli Lilly, Galapagos, GSK, Novartis, Pfizer, Sun, and UCB, and has been a speaker for AbbVie, Amgen, Eli Lilly, Janssen, Novartis, Pfizer, and UCB. AK has received grant/research support from AbbVie, Amgen, AstraZeneca, BMS, Celgene, Centocor-Janssen, Pfizer, Roche, and UCB. AO has received grant/research support from AbbVie, Novartis, and Pfizer, and has served as a consultant to AbbVie, Amgen, BMS, Celgene, Corrona (now CorEvitas, LLC), Eli Lilly, Gilead, Novartis, Pfizer, and UCB. AFW has received grant/research support from AbbVie, Celgene, and Lilly, and has served as a consultant and speaker for AbbVie, Alexion, Amgen, BMS, Celgene, Horizon, Lilly, Novartis, and UCB. MB has served as a speaker for AbbVie, Amgen, Novartis, Pfizer, and Sanofi; has served as a consultant for AbbVie, BMS, Celgene, Genentech, Janssen, Merck, Novartis, Pfizer, and Sanofi; and is a stockholder in Johnson & Johnson. DDG has received grant/research support from and/or served as a consultant for AbbVie, Amgen, BMS, Celgene Corporation, Eli Lilly, Galapagos, Gilead, Janssen, Novartis, Pfizer, and UCB. SR, LT, and SJ are employees of and stockholders in Amgen Inc. JSS has received grant/research support from AbbVie, AstraZeneca, Eli Lilly, Janssen, Merck Sharp & Dohme, Pfizer, and Roche, and has served as a consultant and speaker for AbbVie, Amgen, Astro, Celgene, Celltrion, Eli Lilly, Glaxo, ILTOO, Janssen, Merck Sharp & Dohme, Novartis-Sandoz, Pfizer, Roche-Chugai, Samsung, Sanofi, and UCB.
- Accepted for publication March 29, 2022.
- Copyright © 2022 by the Journal of Rheumatology
This is an Open Access article, which permits use, distribution, and reproduction, without modification, provided the original article is correctly cited and is not used for commercial purposes.
REFERENCES
DATA SHARING POLICY
Qualified researchers may request data from Amgen clinical studies. Complete details are available at https://www.amgen.com/datasharing.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.








{kind=link}
{kind=link}
{kind=link}